
So like no shit, there we were…
Today we went on the PRT (provincial reconstruction team) base in Jalalabad. Lou had arranged the meeting. A New Yorker was running it. He spoke fast (refreshingly so, as one’s mind atrophies from a predominance of interaction with non-native speakers.)
He was excited about a particular new funding stream from USAID that was meant for offbeat projects that are not being addressed by other large funds. Lou had connected a few dots and suggested cricket fields and now the ball is rolling.
During the meeting I was drowning in acronyms. At some point, I requested a time out to deacronymify. I think it was around the point that we were told that the proposal should, of course, address COIN (counter insurgency) objectives.
Here are some notes from that time-out: Â Feel free not to read them!
- PDC (Provincial Development Council) staffed by PC (Provincial Council) who are the voting members, 19 of which 5 are female.
- ASOP — Afghan Social Outreach Program, subset of IDLG
- DDA — District Development Association
- These are all Shura’s of appointed peoples. But the best guys are the rung bellow them, the CDC — community development councils — “They are like the small town PTA (Parent Teacher Associations) in America that know what the local issues are, and they are elected!”
- TWG — technical working group, usually the TWG of some subject under some other acronym.
- IDLG — Independent Directorate Local Governments (a USAID government partner). They appoint local governors, and DDBs (District Development Boards)
- ANDS — Afghan National Development Strategies
- StIKA — Stability in Key Areas. It’s the new LGCD (Local Government Commercial Development).
- NSP (National Solidarity Program) is under the NMRD? WTF?
They did not have a shop at the PRT, but we were able to get some hygienic products at the MWR (Morale Welfare and Recreation) bunk.We had lunch at the DFAC. Over lunch, it was mentioned that USAID is understaffed in the region. I asked where the bottleneck lies. It turns out that there are more USAID employees hanging in Kabul/Bagram ~1200 than are active in the field. And the reason is quite an American one. In practice, USAID employees that are part of the PRT have to be physically fit to ride with full Army gear in MRAPS. (And that is the only way they are allowed to get around to get their work done.) It’s hot and heavy.
As an American company, USAID has to follow the American with Disabilities Act for Hiring, which means that they cannot exclude people based on their level of fitness (sometimes age or disability) for the task at hand. USAID has problems recruiting people that are younger and can get clearance. So their payroll is full of old guys.
The net result is all the physically fit people (600 of them) are active in the field while Kabul is a “geriatric ward” (1200).
“This is your government.”
***
When you live “outside the wire”, going the DFAC (Dining Facility) at the base is kind of like raiding your parent’s pantry when you are a poor student. You fill your pockets with gum, soda, cookies, cliff bars, etc. Here was our score today:

We focused on gum. Â Thanks Uncle Ben!
***
Dave was telling me that when he hung out with the Special Force guys, all of their stories started with, “So like no shit, there we were…”

So like no shit, there we were on an American base playing basketball and trash talking in Russian with our Afghan driver/translator Najib, inside an empty swimming pool, which was initially built by the Russians when this was their Army base and then used by the Taliban as an execution ground. You could see the bullet scars on ground, and the US soldiers would circle around us, doing their business, occasionally recovering our balls which had bounced out of the pool.

***
And to round out today’s ramble is a good one, but you have to click some links. It’s a TAL (This American Life) episode. In the first act you will meet JD (Japanese Dude) — aka Mohammed Jawed. He’s the one that took the photo of the sheep and boy on the bike (earlier post). Well anyways, listen to this act, which is like the first 5 minutes: http://www.thisamericanlife.org/radio-archives/episode/369/poultry-slam-2008
Measure Ma’an
Each be ruled by his own.
Here in Jalalabad, wood is ruled by a ma’an (my spelling, trying to caputure the pronunciation. Elsewhere it is spelled mann.)
Most of the heating and cooking energy needs in Afghanistan are supplied by wood. Along the road you see plenty of shacks of the wood dealers. Â Today we stopped by. Â Typically kids are chopping wood while an older bearded propriator (father/uncle) is sipping tea and waiting for customers.

I noticed our wood was being weighed on a scale, but instead of weights, it was counterbalanced by calibrated rocks. The unit of measure is a ma’an, which varies locally but approximates 7 kilos.

A ma’an is the prefered unit of measure for wood, and is part of a comprehensive unit scale:
|
. |
||||
|
. |
||||
|
. |
ma’an | SI | Typical Items | |
|
. |
||||
|
. |
1 kharwar | 80 | 560 kg | wheat chaff, scrap metal |
|
. |
||||
|
. |
nim kharwar | 40 | 280 kg | |
|
. |
||||
|
. |
1 ma’an | - | 7 kg | wood, rice |
|
. |
||||
|
. |
nimma’an | 1/2 ma’an | 3.5 kg | |
|
. |
||||
|
. |
charak | 1/4 ma’an | 1.25 kg | carrots, onions |
|
. |
||||
|
. |
nim charak | 1/8 ma’an | 625 g | |
|
. |
||||
|
. |
1 pau | 1/16 ma’an | 322 g | lemons, peanuts, sugar, meat |
|
. |
||||
|
. |
nim pau | 1/32 | 219 g | |
|
. |
|
. |
khord | 1/64 | 109 g | henna, chai |
|
. |
||||
|
. |
nim khord | 1/128 | 55 g | |
|
. |
||||
|
. |
pookhtabar | 1/256 | 27 g | herbal medicine |
|
. |
||||
|
. |
nim pookhtabar | 1/512 | 14 g | |
|
. |
||||
|
. |
chitakai | 1/1024 | 7 g | spices, surma |
According to wikipedia the etymology can be traced to the Hebrew word mana, as in mana from the desert. Every day the wandering tribe that exited Egypt was allowed to collect one Omer of mana. On Friday, the collection was doubled, to provision for Saturday, the Sabbath day of rest. An omer is a dry weight of measure, approximately the volume of 3.5 liters of water. On Friday therefore, the collection was 7 volumetric liters, which would weigh 7 kg (if water).
To continue reaching for more connections, the ma’an weights were made of stone. An imperial stone is 6.35kg, not that far off?!
None of this should be confused with a ma’an in Pakistan. A Pakima’an is apparently 7 times an Afghan ma’an.
Not everything is measured using this scale. If for example you were buying opium, then the standard measure is a “kartus” defined as the weight of a AK47 bullet casing, a sensible standard from those at hand.
Shoes
Behold a typical Afghan shoe.

It’s a dress shoe, because that’s the preferred style. And it’s bent in the back because they wear them like slip ons. This is convenient. Afghans take them on and off so many times a day. They take them off to pray 5 times a day. They take them off whenever they enter someones house for tea, etc. etc. And this is probably true across most of Central Asia and many other countries in the “rug belt”.
What I don’t understand, is why no one has seized on this huge market opportunity of making a fancy dress shoe, without a back, a dress shoe natural slip on? (Maybe someone has, and this is your opportunity to market their wares in the comments.)
Another interesting consequence of this, is that there is so much more work for shoe shiners. When you take off your shoes in the restaurant, they walk up and make their offers.

This is a much more natural way to do this than what I have seen in the West. I just couldn’t ever imagine myself sitting down to have someone kneel in front of me to shine my shoes, while I made myself look busy with a newspaper. To bad, I have nothing to shine here. Can you guess why?

I got some army boots from the Bush Market the other day, and while I smelled weed when we walked into the shop, I didn’t expect the shopkeeper to take a mini break to toke on a apple core bong in the process:

Guns and Welding
I was playing around with my stick welding skills when I attracted the interest of one of our security guards. He wandered up, trying to look nonchalant, to check out what I was doing that was making so many sparks. I showed him the section of an ammo case lid where I had ground off the paint and was practicing laying welds.
When he saw I also had a 40mm bullet casing, then he got really excited. He pulled out a clip of live ammunition from his cammo vest and took an AK round out to ask, through gestures and hand signals if what I had was also a bullet. I nodded in agreement and he was hooked. Unfortunately, the bullet casing turned out to be aluminum not steel, but I had acquired my first student.
Meanwhile, during our bullet exchange, Mustafa, the “house commander†joined us. Not wanting to be left out of the fun he picked up my angle grinder and gestured how he should use it, looking to me for a nod of assent. I showed him where the button was and next thing I knew the two guards were grinding all the paint off of my ammo case, prepping it beautifully for lots of welding practice. If we got those two guards into the Boxshop, all our FLG grinding problems would be over. They worked the thing meticulously, getting at every scrap of green paint until the thing shone.
And that’s how I came to teach two Afghan men with very large guns who speak absolutely no English how to stick weld. We’ve arranged for lesson two tomorrow, inshallah, as they say here.
Ladies Night…. Or Afternoon
The park in Jalalabad is, like so many other public venues, open to men only. However, Wednesday is special. Wednesday is Ladies Day.
So Jenn, Kellie and I decided to take a soccer ball and spend a few hours hanging out in the park with the Ladies of Jalalabad. The park is surround by tall walls, shielding it from the views of passersby and the entrance is guarded, per usual, by a young man in fatigues holding an AK-47. He gave us a nod of approval and we slipped through the gate to the other side.
Women on the streets of Jalalabad move quickly and purposefully from one destination from the next, covered in sky blue burqas. They don’t linger on the streets with the men. If lucky you may catch glimpses of red or purple pants or a sparkly dress under the burqa’s cloak, but women are largely anonymous, covered creatures in public.
However, the park on Ladies day, safe from the eyes of men, is an outlet. An opportunity for girls and women to enjoy being outside, uncovered, largely free. They sat in clusters and groups, burqas cast aside, dressed in bright colors with heavy layers of kohl and lipstick painted on. I have no way of knowing if they always are so done up or if the park was an excuse to really dress up, but the golden fields of parched grass were covered in the saturated greens, pinks, reds and purples of the tunics and headscarves of these women.

While their mothers and older sisters sat in the grass, picnicking and drinking tea, hordes of children ran around, screaming, playing, and fighting with one another. When Kellie, Jenn and I starting kicking a soccer ball around and invited some kids to join us we nearly started a riot as the cluster of kids raced after the ball.

The kids also love having their photos taken. The boys especially will preen and strut in front of my lens, trying on different poses and hamming it up. The girls bring forward their baby brothers for photo ops, their way of trying to get captured on film. They’ve been taught they shouldn’t have their photo taken, but if it happens that they are holding a baby who is being photographed and they make it into the shot…..


As we were obviously not Afghans, we garnered lots of attention, not only for our soccer ball and cameras. Young women frequently approached us, chattering away in Pashto, not caring that we had no clue what they were saying. They showed us their babies, offered us tea, and gestured emphatically to get points across that were thoroughly opaque to us. Smiles abounded and we nodded enthusiastically, not knowing what we were agreeing with.
A few men are allowed in the park- they run the food stalls and the photography studio in one corner. For some reason this arrangement is understood as acceptable and the girls pose for photographs and buy ice cream cones with their headscarves down.
However, the guard on duty within the walls was female as well- the first female Afghan security personal I’ve seen. She was a stocky woman in fatigues and black headscarf who brandished her large knife menacingly at kids who appeared to be misbehaving. Unlike every male in fatigues, she had no gun.
After a few hours of enjoying the sunshine we said our goodbyes to new friends, promised to return next week, covered up our hair once more, and passed back onto the street, back into the realm of men.
Coming to Terms
And there’s more where these came from…


Kabul to Jalalabad
The ride from Kabul to Jalalabad was long and adventurous.
I saw a dog being killed in Kabul. They are considered pests here.

Most of our drive time was spent sitting in traffic on the windy segment of the Kabul River Gorge (also called Tangi Gharu).
Part of the reason for the bad traffic is that people tend to drive on both sides of the road in both directions. At first it seems like a good idea, you get a little bit ahead of your neighbor. But local optimization can sometimes lead to global catastrophes. Such decisions created gridlocked jenga puzzles on narrow roads with precarious drop offs and small margins for error. Each one took hours to resolve.

Had we left much earlier in the morning (say 6am) we wouldn’t have experienced this traffic. And so we sat in the car, or got our to stretch our legs, or to take photographs of war debris from various wars, such as this Russian tank:

Whenever we’d show our faces, a crowd would appear. The younger ones talked to us. Sometimes they asked for “energy” = soft drinks.

I met a boy named Pamir who is studing law, on the right. He’s gonna be a bureaucrat some day. On his student card, you could see his blood type.
Jingle Trucks from Parkistan constitute a large fraction of the traffic:


Out of the gorge we were out in broad open valley swept by opaque dust storms, bending trees horizontally.
The road had warn away in parts, and you have to be ready to stop abruptly when you spot a pot hole. This caused our accident. A truck in front of us stopped. We stopped right behind it, and many cars stopped on our bumper behind us… So far so good. But the truck in front started backing up. We honked. It didn’t care. It ate half our hood before it finally stopped.

Thankfully, its clearance was high enough that the damage was only cosmetic. Since there is no insurance and no protocol for how to resolve accidents other than by talking. Our driver (on the right) got out and started a long negotiation directly on the highway. (Truck driver is on the left.)

This is one of the main reasons why foreigners are discouraged from driving. All of the NGOs and even the security companies now hire local drivers. This is the kind of advice we get: if you hit someone, get the hell out of there. If you stick around, you will get clubbed. (And if you see someone dead/wounded, look out for booby traps. This one applies not only while driving.)
One amazing thing about Afghanistan is the jusxtaposition of the past and the future, and how one causes the other. Â There is no postal service, for example. Â You have to rely on email.

There will probably never be a wired telephone network here, but everyone has a cellphone. Cellphone towers (when not powered by generators) are powered by solar.
We did see construction crews laying fiber optics cable along the highway. Sadly, I missed the photo op. Maybe Lou or Todd got it?
Much of the country’s hydroelectric facilities are located along this stretch of river, so the fact that the Kabul river is but a stream, presents a problem.

Approaching Jalalabad, we pass the Darunta Dam and aftewards is Nangahar University whose initial buildings were used to house the Soviet engineers that built and operated the Darunta Dam.
Right before you breach the perimiter of Jalalabad city proper, take a left down Awesome Todd’s road (see Open Street Maps).
Welcome to the Taj. This has become our home (Langton Annex 😉 More about the Taj and its occupants in another post.
For now, a teaser:
This is part of the longer narrative blog series, that started with What is Normal anyway? I will try to have this sub-series follow a liner narrative, while the general post stream will jump around.
Hardware Shopping
As it turns out, Jalalabad has no Home Depot. Not even an ACE Hardware. So, when I wanted to purchase an arc welder  to make furniture and art out of old ammo cases and bullet casings, Mehrab took me and Peretz to the bazaar. More specifically, to the hardware store section. Jam packed stalls nestled next to one another, crammed and overflowing with jumper cables, machine belts, rusty bolts, and cheap Chinese screw drivers. Functioning as individual isles of the larger bazaar,  the coexisting shops all stock many tools while each specializing in a few. A customer starts a relationship with one owner, who then sends runners from their staff to other shops along the way to grab any items not in stock. We choose a shop, out of accident more than reason, and began the process of buying tools.

First, we collected assorted wrenches, hammers, and screwdrivers, gesturing “bigger,†“smaller†or “heavier†to suit our needs. We perused the single aisle, avoiding the pair of chickens roosting under the fully stacked shelves. Angle grinder. Leather gloves. Welding goggles. Check. Our shopkeeper showed us a file and told us it was “Good quality. Made in India.†Even Afghans have disregard for cheap Chinese made tools, although the store was still full of them. The quality products they see come from India, hopping over Pakistan to compete with inferior goods.
Then onto the reason we were there: a welder. The shop sold one option, a red metal box with 5 thick screws protruding, announcing the amps they would draw, and a grounding screw sticking out the side. Instead of a power cord, two bare wires extended, ready to be stuck directly into a socket, as is the local preferred method of “plugging in†an appliance. However, for this compact metal box to be useful as a welder we needed to piece together its attachments. The store sold us eight meters of heavy duty wire, cut off a large yellow spool. Next, we debated the merits of the two options for handles and settled on a heavy duty grip. But when I inquired about a grounding clamp, vitally needed to complete a welding arc, our shopkeeper seemed perplexed. He sent one of the boys lingering in the shop off to find one, while he encouraged us to drink some chai. We perched on tanks of gas and sipped steaming hot cups of sweetened, cardamom flavored tea until the boy returned, with a pair of jumper cable clips. Not exactly what I had in mind, but it’d do.

The bits and bobs added up to most of what would be needed or useful for arc welding and so, as we paid the shopkeeper, our tools and supplies were loaded into a wheelbarrow for transport. Next step: assembly and testing of the MacGyver welder.

Nangahar Public Hospital
The first time we came to the hospital, the staff apologized profusely for not being able to host us. They were dealing with the wounded of a suicide bombing incident in the district. There was one casualty. Five people were in the OR. And they were embarrassed in front of us, that such things happen in their country. We left, and came back yesterday.
Nangahar Public Hospital (NPH) is a Regional Post-Graduate Teaching Hospital for the Eastern Region of Afghanistan. The Eastern Region covers the provices of Kunar, Nangahar, and Laghman. But in practice it also covers the provinces of Logar and Kapisa, and the district of Sirobi (which technically belongs to Kabul Region).
22 clinics from the Eastern Region transfer patients to NPH by ambulance. The hospital does not have an Emergency Response Ambulance team. Three district hospitals of Kama, Ghaniki and Khugiani also refer patients to the NPH.
Location. The hospital is located in the city of Jalalabad, halfway between Peshawar and Kabul, on the main highway linking the two. This highway is the main transport/supply line between Pakistan and Afghanistan. The border checkpoint, called Torkam Gate, is a half hour to the East and is the entrance to the Khyber Pass. The stretch of highway west to Kabul is considered the most dangerous road in the world by the NYT. It is dangerous because of accidents. And often, because of accidents, traffic on the narrow road comes to a complete stop. NPH sees 600 patients from car accidents each month. Some patients prefer to be referred to NPH rather than hospitals in Kabul because, if the issue is sufficiently critical, it is a much closer drive to Peshawar, Pakistan where there are hospitals better than anything in Afghanistan.
The hospital has 10 departments, which all train post-graduate specialists: Internal Medicine (Medical Ward), TB, Infectious Disease, Pediatric, General Surgery, Orthopedic, OBGYN, ENT (Ear, Nose and Throat), Opthamology, Neuropsychiatric (opened this year.)
A post graduate medical specialist is someone who has graduated a seven year medical program, CONQUER EXAMINATION, like SAT that determines which Faculty at which University you can attend: The order of RANK based admission by faculty follows: Medical, Engineering, Economics, Law, Agriculture, Computer Science, Literature, etc. So to get to medical school in the first place, they needed top marks. — According to Ahmed “Zia” Ahmedi Here Afghan students vent about higher education on Facebook.served a 2 year practical at a regional clinic, and received high marks at a central examination in Kabul. Based on their grades and specialty of interest, they are sent to post-graduate training hospitals around the country. Most specialists train for 3 years, OBGYN is 4 years, and surgery is 5 years.

According to Alhaj, Alhaj means that he has performed several pilgrimages to Mecca. Â If it were just one, he would be merely Haji. Prof. Mohammad Ismail “Alam”, Chief of Medical Ward, there are 30 specialists being trained in the internal medicine department now, and 15 faculty. (By contrast, there are 3 trainees in the neuropsychiatric department, having started just this year.) The Medical Ward has 15 beds in the ICU/CCU. 8 for women and 7 for men. There are 12 nurses, 6 female and 6 male, and 1 head nurse. In the ICU and CCU both men and women take care of patients of both geners. There are also special wards where female nurses take care of female patients.


Prof. Alam first studied to be a doctor in the 1970s from an American NGO called CARE/Medico. CARE/Medico in Afghanistan — I cannot understand how a writer of Carl Edgar Law’s calibre could have possibly researched health care in Afghanistan and, more particularly, medical teaching there over the past two decades (Can Med Assoc J 1983; 128: 186–190) without discovering the work of the medical service arm of CARE known as CARE/Medico.From 1963 to its dissolution in 1979 CARE/Medico carried out a 3‑year residency program for recently graduated Afghan doctors from the University of Kabul. This program’s nucleus was a permanent team — including a Canadianstaffed laboratory in Avicenna Hospital, Kabul — supplemented monthly by volunteer specialists from the West, mainly Canada and the United States. It was Afghanistan’s only continuous medical teaching link with the Western World.During its 15-year existence (terminated by the Russian occupation of the country, like the Management Sciences for Health program) this teaching course was, in effect, a high-grade residency program in medicine, surgery and gynecology.Probably more than 100 young Afghan doctors became proficient in Western medical and surgical teaching and techniques. There was also a nurse’s training program. So thorough was it that shortly after my return from Kabul in 1968 (having served in the CARE/Medico program there as a teacher) I met one of my students, who had just qualified as a second-year resident at St. Paul’s Hospital, Saskatoon.This may not seem remarkable unless you remember (as mentioned in the CMAJ article) that the University of Kabul’s medical school taught “archaic” medicine in French that was simultaneously translated into a Farsi dialect, which is pretty well devoid of medical equivalents.I feel that Mr. Law’s article was informative — but only on a small segment of the subject. Canada’s contribution in expertise and manpower (doctors, nurses and laboratory technicians) to this Afghanistan program was outstanding and should be duly recorded.FRANK MACINNIS, MD, FRCP©, FACP; Clinical director; Department of Psychogeriatrics; Alberta Hospital; Edmonton, Alta. (source: PubMed)Â He fondly remembers Dr. Mobri (first name and not sure about spelling) who taught him, and wonders if he can get in touch with him now. The American staff left the CARE/MEDICO internal medicine training clinic when the Russians came, and Prof. Alam stayed there for 13 years (whole time of the Russian occupation) leading the clinic. He said that the Russians kicked out the Americans and treated the CARE/MEDICO trainees with scepticism, accusing “Alam” of being a CIA agent. “When the Russians left and Mujuhadeen came to power and there was unrest in Kabul (early 90s) I left on a fellowship to India. And when I returned a few years later to the Taliban, I transfered to Nangahar Public Hospital and have been here ever since.”

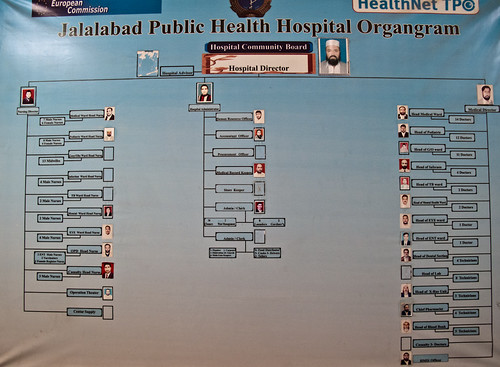
Most hospital buildings were initially built by Russians. For a while, the Red Cross of New Zeland supported the surgery departments. Now the whole hospital is managed by HealthNET TPO, an NGO based in Holland, and funded by the European Commission. The hospital is owned by the Government, but HealthNET manages it and pays for all patient services as well as all 545 staff of the hospital from Security Guards (whose pay starts at 5000 Afs = 100$ per month) to Nurses (7.5–10k Afs=150–200$/month) to Doctors (12–20k Afs=220–400$/month) to Administrators (~15k Afs = ~300$/month).

Ahmed “Zia” Ahmedi is the hospital administrator employed by HealthNET TPO. He is 28, energetic, and speaks almost perfect English, which he learnt in Pakistan, where he spent the first 22 years of his life. He sports an iPhone 3GS which rings non-stop. He jokes, “I am like the telephone switch board.” He moved to Kabul six years ago to work for the UN, then switched to work for a US State Department Justice Support Initiative, and then as an administrator for the International Medical Corps. But he likes his current job at the hospital most, because he sees the people he helps.

Zia says that the biggest problems with hospital are social. Patients fight with doctors, neglect health codes, and barge into Operating rooms during surgery. “They are unfamiliar with hospital conduct.”
*** READ ON FOR THE GRITTY DETAILS ***
Please forgive the current look, I have to clean up this formatting.
Nangahar Public Hospital Visit (01/04/11Â — 10AM — 3:30PM)
Lou and Peretz visited the hospital to inspect equipment, meet staff, and assess needs.
Met:
- Ahmed Zia Ahmedi, Hospital Administrator
- Dr. Baz Mohammad, Hospital Director
- Alhaj, Prof. Mohammad Ismail “Alam”, Chief of Medical Ward
- Nurse of Medical Ward
- Doctor from Surgical Ward
- Almas (stayed for first hour)
- Qahar, Internet Facilitator of Medical Faculty, accompanied us until lunch.
Places:
- Admin Offices
- Medical Ward — ICU/CCU
- Surgery Ward — Post Op Recovery Men/Women
- Equipmnent Storage
Equipment Inspected:
- Bed Side Patient Monitors — Philips SureSigns VM8
- 1 in Storage — missing cables — apparently Rotary and AI crew already know about this and are bringing the needed cables. Is this correct?
- Ed Myers — 1 unit in storage should not be a Philips Patient Monitor email indicates the locations — Maybe it shouldn’t, but it is: http://www.flickr.com/photos/49543096@N03/5327332655/ From the locations email vs what we have seen, this is probably the free standing one from the Operating Theater. We will make a point to track down cables. Then again, in the photo all of the cables appear to be there. We’ll figure out what to do with it and report back!
- 9 in Medical Ward (All working. Sticky electrodes — apparently HELBIG doesn’t work, but PLIA-CELL DIAGNOSTIC ones do work.)
- Ed Myers-Some of the ekg stickys are for the 12 lead EKG machine so this is true
- Is the 12 lead EKG in storage? We saw two GE ECG machines (see below)
- Ed Myers-Some of the ekg stickys are for the 12 lead EKG machine so this is true
- 2 in Surgial Ward (One missing the blood pressure cuff. They don’t have any    sticky  leads.)
- Ed Myers- ICU/CCU has supplies for entire hospital and they must share since this is where we put the supplies so the hospital would have a central supply room. This should help for accountability re ordering etc Great!
- Did not inspect 1 in Gynocology and 1 in Pediatrics, but reports are they are working.
- 1 in Storage — missing cables — apparently Rotary and AI crew already know about this and are bringing the needed cables. Is this correct?
- 2 Older Patient Monitors (Medical Ward) “Broken”
- First unit MEC-1000 missing fuse (“T1.6A” outside or “5TT 1.6A 250V ul” on old working fuse.) They bought replacement fuses, which do not work. This may be because they purchased a 10A fuse, which still fit the socket. I currently have the old broken fuse and the replacement fuse they got. Any ideas on where to look for replacements?
- Ed Myers- I left fuses for the Philips monitors they are T1.6amp, head nurse knows where they are they where left for eng Storrs. We only met him briefly then disappeared. Also left were memory sticks with latest software that i installed. These stick also contain manuals/guides. You might want to look at them if you have the time. > Great!
- Second unit GT9000 seems to work, but is missing cables. Appartently this is because the cables are now in Kabul with the person who is shopping for more cables. This is a good thing.
- First unit MEC-1000 missing fuse (“T1.6A” outside or “5TT 1.6A 250V ul” on old working fuse.) They bought replacement fuses, which do not work. This may be because they purchased a 10A fuse, which still fit the socket. I currently have the old broken fuse and the replacement fuse they got. Any ideas on where to look for replacements?
- 2 ECG Machines (Storage — awaiting deployment) — GE Mac 5000
- One battery (GE MAC PAC 18V 3500mAH NiMH, GEMS-IT P/N:900770–001) seems to be defective. Unit works when plugged into wall, but when unplugged, the charge holds for ~ one minute. We swapped batteries between units and confirmed that this is a battery rather than a unit/charger issue. If this cannot be locally sourced, one possibility would be for us to open up the battery case and replace the internal NiMH batteries with ones that we probably can purchase here.
- Any input?
- Second battery works fine. Both units are now in storage, awaiting distribution. Medical Ward wants one. Actually they want both.
- Brad says, one was shipped without connectors but connectors are coming.
- One battery (GE MAC PAC 18V 3500mAH NiMH, GEMS-IT P/N:900770–001) seems to be defective. Unit works when plugged into wall, but when unplugged, the charge holds for ~ one minute. We swapped batteries between units and confirmed that this is a battery rather than a unit/charger issue. If this cannot be locally sourced, one possibility would be for us to open up the battery case and replace the internal NiMH batteries with ones that we probably can purchase here.
- 1 BiliBlanket Transilluminator (Storage) — Which they thought was a broken UPS and now that they know what it is, are unsure what to do with. Apparently this is used in neonatal wards for infant light therapy (to treat/prevent jaundice) and as a transilluminator in helping locate veins for IV. We can explain this to the doctors, but perhaps this will require a training demonstration. MedWeb?
- 1 Ohmeda Medical Phototherapy (Storage) — Also for treating neonatal Jaundice — Missing bulb and internal cables. Apparently Rotary and AI crew is aware of this and will bring needed parts. Is this correct?
- Ed Myers- this is correct unit needs a new bulb it blew out wiring should be okay. Brad is more familiar.
- Almas and Qahar (the IT guy) said they know what to do with the part once they get it.
- Ed Myers- this is correct unit needs a new bulb it blew out wiring should be okay. Brad is more familiar.
- 1 Difibrillator (Storage) — “We have theoretical knowledge how to use it and think it works but we have not yet had a patient who has needed it.“ I neglected to inquire why it is in storage, rather than at a location where a patient might need it. This is an interesting point that they do not have patients that need it. Does it mean that by the time they get to hospital, they no longer need it? Would a training session be helpful to encourage its use? Medweb?
- Ed Myers- I am sure they will need it someday, no comment, it should always be plugged into power to keep battery charged and close to patients for when it is needed. It is a short period of time between V‑fib and death.. Dr Steve can comment
- We will make sure to relay this information. Where would be a good place to keep it?
- Ed Myers- I am sure they will need it someday, no comment, it should always be plugged into power to keep battery charged and close to patients for when it is needed. It is a short period of time between V‑fib and death.. Dr Steve can comment
Summary of Requests:
- Medical Ward wants more patient monitors. They have 15 beds. 9 new monitors. 2 old, under repair. Want 4 more. Actually they want 6 more new ones ;) This doesn’t need response. It’s just for the record.
- Medical Ward wants ultrasound machine (which the doctor called it a “doppler machine”.) The current one is located in Gynocology Ward. Zia suggested that it was too heavy to move and so it has remained in gynocolgy. Probably this is an internal issue of the hospital and not our issue, but nevertheless recorded. This doesn’t need a response. Just for the record.
- Medical Ward wants help getting new fuses for patient monitor. Solved
- Surgical Ward needs sticky electrodes for patient monitors. I suggested that they start by asking the Medical Ward to share. (They did not know the Medical Ward had any. Zia said he will assist with this.) Solved
- Surgical Ward needs a blood pressure cuff for a patient monitor which is missing one. (Did it go missing during installations?)
- Ed Myers- The ICU/CCU area has a cuff for this monitor Great!
- New MAC PAC battery for the GE MAC 5000 Portable ECG?
- Hospital Administration wants internet. They currently have intermittent internet. Zia said when it works it is very slow and it’s often out for up to a few weeks at a time. (Is it Fab Fi? They seemed to suggest so.) He stressed how important this is, “more important than anything else.” They have emails and things to look up, partient records, medical info, but often cannot do so. Zia says there is internet in MedWeb Room that Almas knows about, but that it is not shared around. Will ask Almas about this, but perhaps someone else knows about this also?
- It may be that new NATO funded internet which is going up at teaching hospital will cover them too. Anyone can confirm?
Recommendations:
It would be really convenient to have a Radio Shack in town, to grab fuses and such. It’s far less optimal to have to source things from far away, in terms of time, money and sustainablity. It would be good to source items locally. Perhaps we can help jump start a local distributor business by guaranteeing their inventory investment (say starting with good UPSs, fuses, EKG electrodes, …) their job will be to keep track of where to source such items when necessary and carry an inventory of the most frequently used items. Can you please help assess the merits of such an idea?
Ed Myers- divine intervention on may home from amsterdam the last night I met a Philips person in the hotel reception are who handles this part of the world. This is a great idea for a start up or see if this group is an opportunity that allready exist. I will send this email tonight. Thank you Ed, I will make sure to follow up.
Transport:
— IN: Salahudin (Mehrab’s nephew and his assistant at the Taj)
— OUT: Mr. Dawood, who says hello to all of the Rotary and AI crew he had transported previously!
We are having problems getting around and have to beg for rides. We would be more effective if we had a more reliable arrangement with a driver that we can call and pay to give us rides. Any suggestions?
***
Question to Fary — Is there yet another place where equipment is stored and not used? In a previous email you referred to “for example, US military purchased $450.000.00 worth of equipments sitting in the corner of room and dusting because they do not know how to use them.“ I was not able to locate this with questions alone. Also, according to your estimations which equipment do the doctors need training with (but will not admit it)? I could use some advice as to how to probe. Perhaps it is in the teaching hospital? We have met with Dr. Khan today but did not complete the inspection. “The person with the key” was not around. We are coming back on Saturday.
Question to Steve Brown — Qahar said you had a plan to make a Medical Library. Could you share some details of the project? I have brought many (and have access to more) ebook textbooks on different subjects (science, engineering, agriculture, ESL, etc.) and talked to Qahar about hosting this data on the local network at the Medical Faculty.
Idea — Can negotiate free PubMED access?
Soccer with the Boys
The cook scored 3 goals. The mechanic Sadik stayed in goal. The guard Metin scored 7. I scored 9.
